
1. What is JIA?
Juvenile idiopathic arthritis (JIA) is a chronic, pediatric autoimmune inflammatory arthritis characterized by the presence of synovitis with associated joint pain, warmth, swelling, and/or decreased range of motion to a joint. Arthritis must be present for at least 6 weeks in a child with symptom onset prior to the age of 16 years, not explained by any other cause. It is associated with decreased joint mobility, growth disturbances, and irreversible joint damage. JIA affects 1 in 1000 children in the United States. There are 7 different subtypes:
- Oligoarticular
- Polyarticular Rheumatoid Factor (RF) negative
- Polyarticular RF positive
- Enthesitis-Related Arthritis (ERA)
- Psoriatic
- Undifferentiated
- Systemic*
*Systemic JIA is different than other subtypes of JIA and is more of an autoinflammatory, rather than autoimmune disorder. It most closely resembles Still’s disease in the adult population. It is characterized by arthritis in one or more joints and fevers for greater than 2 weeks that occur daily for a minimum of 3 consecutive days and one or more of the following 1) evanescent rash, 2) generalized lymphadenopathy, 3) hepatosplenomegaly, 4) serositis.
2. Key Signs and Symptoms
- Oligoarticular (2 types – persistent and extended)
- Persistent: 4 or less joints involved during the disease course
- Extended: when more than 4 joints are involved after the initial 6 months
- Mostly affects kids between 1-3 years old
- Typically affects the lower extremities, leg length discrepancies (LLD) are common
- Polyarticular RF negative
- Arthritis affecting 5+ joints
- RF antibody testing is negativePeak age of onset is 1-3 years and then 9-14 yearsKnees, ankles, and wrists are commonly affected
- Most likely to have temporomandibular joint (TMJ) or cervical spine involvement, jaw deviation can be a helpful clue
- Polyarticular RF positive
- Arthritis affecting 5+ joints
- RF antibody testing is positivePeak age of onset 9-11 years
- Can affect large joints of upper and lower extremities
- Most commonly involves small joints of bilateral hands, which cause various kinds of deformities
- Enthesitis-Related Arthritis (ERA)
- Must have arthritis AND enthesitis
OR
- Arthritis OR enthesitis with ≥ 2 of the following:
- Sacroiliac (SI) joint tenderness
- HLA B27+Onset in boy >6 yearsFamily history of HLA B27+ diseases
- Acute symptomatic anterior uveitis
- Psoriatic
- Must have arthritis and psoriasis OR
- Arthritis and 2 of the following:
- Dactylitis
- Nail pits or onycholysis
- 1st degree relative with psoriasis
- Undifferentiated
- Does not completely meet criteria for one of the previous categories OR
- Meets criteria for more than one category
Associated conditions: uveitis, inflammatory bowel disease, psoriasis
3. Risk Factors
- Genetic:
- Family history of autoimmune disease
- HLA-B27 and other HLA alleles
- Environmental:
- Viral or bacterial infections
- Trauma
- Demographic:
- Age: onset before 16 years old
- Sex: prevalence higher in females
- Lifestyle:
- Psychosocial stress
- Obesity
- Secondhand smoke exposure
4. Diagnosis
JIA is a clinical diagnosis based on history and a physical exam. There is no specific diagnostic test.
- Labs
- ANA, RF, CCP, HLA B27 – used to assess prognosis and risk of uveitis
- ESR, CRP – inflammatory markers, which are typically not elevated in most subtypes
- Ferritin – if systemic JIA is suspected
- CBC with differential, CMP
- Other labs to consider for ruling out other possible etiologies of joint swelling
- Transglutaminase IgA, Serum IgA – celiac disease screening
- Stool calprotectin – IBD screening
- B. burgdorferi antibody with reflex – Lyme disease screening
- TSH, free T4 – thyroid disease screening
- Vitamin C – scurvy screening
- Imaging
- Xrays – more useful for determining presence of chronic arthritis and damage such as bony erosions
- MRIs (w/wo contrast) – helpful for assessing presence of both active and chronic arthritis
- Clinical criteria: joint swelling, decreased range of motion, increased warmth, tenderness, flexion contractures, growth disturbance (i.e. leg length discrepancy)
5. Treatment Goals
- Preserve joint function and range of motion
- Enable full participation in school, sports, and all daily activities
- Promote highest possible quality of life
- Support normal childhood growth and development
- Achieve and maintain clinical remission
- Control pain and inflammation
6. Medications
- Symptom Relief:
- NSAIDs
- Intraarticular corticosteroid injections
- Conventional / Foundational:
- Methotrexate (PO or SQ)
- Biologic Therapies:
- TNF inhibitors: etanercept, adalimumab, infliximab, golimumab
- IL-6 inhibitors: tocilizumab
- IL-17 inhibitors: secukinumab
- IL12/23 inhibitors: ustekinumab
- T-cell co-stimulation blocker: abatacept
- Targeted Synthetic Therapies:
- JAK inhibitors: tofacitinib, upadacitinib
7. Management & Nursing Considerations
- Physical Activity & Lifestyle:
- Encourage exercise and weight management
- Counsel against excessive rest, which may worsen joint stiffness
- Educate that inflamed joints are at risk for injury, so focus should be on low-impact activities like swimming or walking
- Patient Education:
- Educate how to administer subcutaneous injections
- Discuss importance of taking medications as prescribed
- Teach patients and families how to recognize signs of disease flare
- Discuss how JIA may affect school attendance, performance, and social activities
- Monitoring:
- Monitor disease activity
- Assess for adverse effects of medications
- Routine medication monitoring labs (q3 months)
- Repeat imaging studies as necessary
- Regularly assess the child’s growth and development
- Emotional Support:
- Provide emotional support during visits
- Ensure patient is connected to interdisciplinary mental health services
- Involve child life, if available
8. Definitions & Key Terms
- Synovitis: inflammation of the synovium, the connective tissue that lines the joints
- Enthesitis: inflammation to the attachment point of tendons and ligaments
- Psoriasis: an autoimmune inflammatory disorder of the skin characterized by erythematous plaques with silver scaling
- Dactylitis: diffuse swelling of the soft tissues of a finger or toe
- Onycholysis: separation of the nail from the nail bed
- Uveitis: eye inflammation, often asymptomatic
- Leg length discrepancy: when one leg grows longer than the other as a result of chronic joint inflammation in the affected extremity
9. Documentation Essentials
- Presenting symptoms
- Medication history and adherence
- Comorbidities
- Physical exam
- Med start/stop dates
- Disease severity scores (JADAS- Juvenile Arthritis Disease Activity Score)
10. Triage Questions
- Which joints are affected?
- Is there just pain or also swelling?
- Is there morning stiffness and how long does it last?
- Any preceding illnesses or injury/trauma?
- Medications tried?
- Impact on daily activities?
11. Nurse Role
The rheumatology nurse plays a crucial role in the care of children with JIA by providing patient/family education, medication monitoring, psychosocial comfort, and assisting with coordination of interdisciplinary care.
12. References
Hersh, A. O., & Prahalad, S. (2017). Genetics of juvenile idiopathic arthritis. Rheumatic diseases clinics of North America, 43(3), 435–448. https://doi.org/10.1016/j.rdc.2017.04.007
Petty, R.E., Laxer, R.M., Lindsley, C.B., Wedderburn, L.R., Mellins, E.D., & Fuhlbrigge, R.C. (2021). Textbook of Pediatric Rheumatology (8th ed.). Elsevier Inc.
Silbert-Flagg, J., & Busch, D. (2025). Pediatric nurse practitioner certification review guide: Primary care (8th ed.). Jones & Bartlett Learning.
13. Pictures
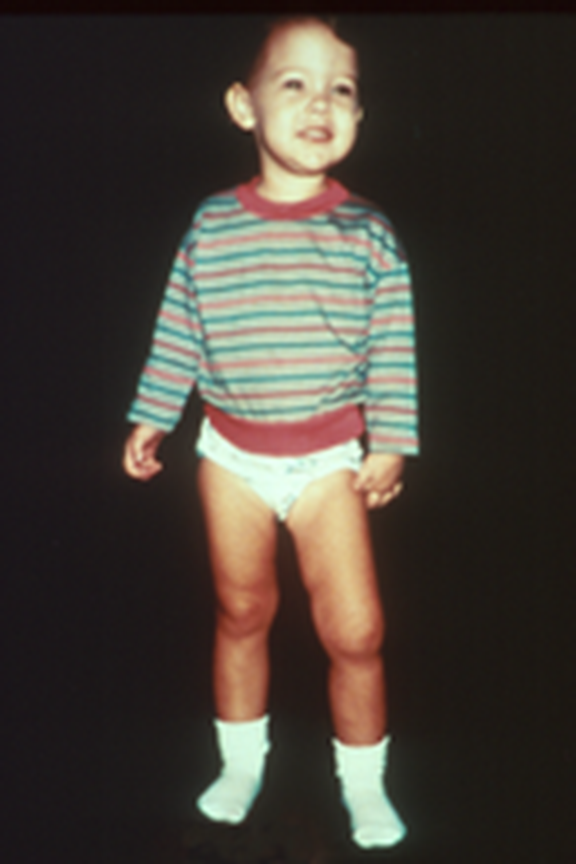
Child with leg length discrepancy

Child with dactylitis

Example of nail pitting

Example of onycholysis
All above pictures were obtained through the American College of Rheumatology Image Library
Contributor: Amanda Karam, DNP, APRN, CPNP-PC
Last Reviewed: March 2026